Curriculum Vitae
Selected 18 Publications
Selected 18 Publications (PDF)
Kimura vs Warshaw Techniques
Spleen-Preserving Distal Pancreatectomy (SPDP)
- Comparison of the Kimura and Warshaw Techniques and Surgical Strategy -
Keywords:
Spleen-preserving distal pancreatectomy; splenic vessel preservation; Kimura technique; Warshaw technique; splenic function
Wataru Kimura, MD,
PhD, Hospital Preident, Tokyo Metropolitan Kasukabe Hospital, Japan
Abstract
In spleen-preserving distal pancreatectomy (SPDP), the Kimura and Warshaw techniques show comparable major perioperative outcomes. However, splenic perfusion-related complications-including splenic infarction, gastric varices, and secondary splenectomy-occur less frequently with the Kimura technique. For benign or low-grade malignant pancreatic lesions, prioritizing splenic vessel preservation using the Kimura technique whenever feasible represents a rational strategy to maximize long-term clinical benefit.
Background
Spleen-preserving distal pancreatectomy (SPDP) has been established as a surgical option for benign or low-grade malignant pancreatic tumors, allowing avoidance of infectious risks and immunological consequences associated with splenectomy. Two main techniques are employed: the Kimura technique, which preserves the splenic artery and vein, and the Warshaw technique, which divides these vessels and relies on short gastric vessels for splenic perfusion. With the widespread adoption of minimally invasive approaches, including laparoscopic and robotic surgery, renewed attention has been directed toward appropriate indications and long-term outcomes of these two techniques.
Purpose
This review aims to compare the Kimura and Warshaw techniques in SPDP, focusing on short- and long-term complications related to splenic perfusion and preservation of splenic function, and to discuss optimal surgical decision-making based on recent evidence.
Previous Reports (Evidence)
Recent systematic reviews and meta-analyses have demonstrated that major perioperative outcomes-such as Clavien-Dindo grade ?III complications and mortality-are generally comparable between the two techniques. In contrast, splenic perfusion-related events, including splenic infarction and formation of gastric collateral circulation or gastric varices, are consistently reported to be significantly less frequent with the Kimura technique. International multicenter retrospective studies further indicate that although long-term survival is equivalent, splenic-related complications are more common after the Warshaw technique. These findings support a strategy favoring splenic vessel preservation for benign and low-grade malignant lesions.
Specific Outcomes Related to the Spleen
1. Splenic Infarction
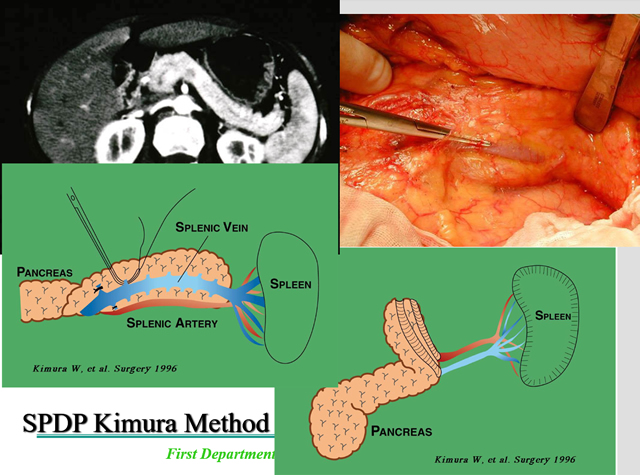
In the Warshaw technique, splenic perfusion depends on the short gastric vessels, which may be insufficient in some patients, leading to a higher incidence of postoperative splenic infarction. In contrast, preservation of the splenic artery and vein in the Kimura technique ensures adequate parenchymal perfusion, resulting in a significantly lower incidence of splenic infarction.
2. Gastric Varices (Collateral Circulation) Development of collateral circulation following division of the splenic vein may lead to delayed formation of gastric varices. Multiple comparative studies and meta-analyses have shown a significantly higher incidence of collateral-related events after the Warshaw technique, highlighting the need for long-term surveillance.
3. Secondary Splenectomy
Secondary splenectomy due to splenic infarction or recurrent splenic complications has been reported more frequently after the Warshaw technique. In contrast, preservation of splenic blood flow in the Kimura technique results in a higher rate of splenic preservation and avoidance of secondary splenectomy.
4. Immunological Splenic Function
The spleen plays a critical role in immune responses against encapsulated organisms. Preservation of splenic function is therefore important for preventing overwhelming post-splenectomy infection (OPSI). Beyond morphological preservation, maintenance of splenic blood flow is considered essential for immunological function, providing a theoretical advantage for the splenic vessel-preserving Kimura technique.
5. Robotic Surgery
Recently, various technical refinements have been reported for robotic SPDP using both the Kimura and Warshaw techniques. Furthermore, a strategic approach in robotic surgery has been proposed: the surgeon should initially attempt the Kimura technique, convert to the Warshaw technique if splenic vessel preservation proves unfeasible, and consider splenectomy only as a last resort.
Discussion
Taken together, current evidence indicates that while both techniques ensure procedural safety in SPDP, the Kimura technique is clearly superior with respect to qualitative long-term outcomes related to splenic perfusion and function. Advances in minimally invasive surgery now enable splenic vessel preservation even under laparoscopic or robotic assistance, supporting the Kimura technique as the first-line approach whenever technically feasible. When severe inflammation, dense adhesions, or vascular proximity preclude safe vessel preservation, the Warshaw technique remains a valuable alternative to avoid splenectomy. However, careful postoperative imaging assessment and long-term follow-up are mandatory, given the risk of splenic perfusion-related complications.
References
1. AL.Conservation of the spleen with distal pancreatectomy.Arch Surg. 1988;123(5):550-553.
2. Warshaw AL.Distal pancreatectomy with preservation of the spleen. Surg Gynecol Obstet. 1989;168:239-243.
3. Kimura W, Inoue T, Futakawa N, et al. Spleen-preserving distal pancreatectomy with conservation of the splenic artery and vein. Surgery1996;120(5):885-890
4. Kimura W, Yano M, Sugawara S, et al.Spleen-preserving distal pancreatectomy with conservation of the splenic artery and vein: techniques and its significance.J Hepatobiliary Pancreat Sci. 2010;17:813-823.
5. Granieri S,Bonomi A, Frassini S, et al. Kimura's vs Warshaw's technique for spleen preserving distal pancreatectomy: a systematic review and meta-analysis of high quality studies. HPB(Oxford).2023;25:614-624.
6. Paiella S, De Pastena M, Korrel M, et al.(2019) Long term outcome after minimally invasive and open Warshaw and Kimura techniques for spleen-preserving distal pancreatectomy: international multicenter retrospective study. Eur J Surg Oncol45:1668-1673, 2019.
7. Takagi K, Yoshida R, Yoshida K, et al. Robotic Spleen-Preserving Distal Pancreatectomy with Preservation of Splenic Vessels Using the Gastrohepatic Ligament Approach: The Superior Window Approach in the Kimura Technique. Digestive Surgery 39 (4): 137-140、2022
8. Kotsifa E, Festen S, Busch OR, et al. Robotic Spleen-Preserving Distal Pancreatectomy: The Warshaw and Kimura Techniques. J Vis Exp, 2024 Jul 26:(209). doi: 10.3791/65216.
9. Lin X, Lin R, Lu F, et al. "Kimura-first" strategy for robotic spleen-preserving distal pancreatectomy: experiences from 61 consecutive cases in a single institution. Gland Surgery 10(1), 186-200, 2021, doi: 10.21037/gs-20-576
Figure Legend
1.SPDP Kimura Methods
2.Wataru Kimura and Andrew L Warshaw in Athens, Greece, 1990.
(At the IASGO international congress in Athens, Professor Warshaw of Harvard University had already published the Warshaw technique for spleen preservation. My publication of the Kimura technique in the English journal Surgery followed six years later.)
Kimura vs Warshaw Techniques
Structured Abstract
Tokyo Metropolitan Kasukabe Hospital
Hospital President
Wataru Kimura, MD, PHD
Background
Spleen-preserving distal pancreatectomy (SPDP) has become an established procedure for benign and low-grade malignant pancreatic tumors, aiming to avoid infectious and immunological risks associated with splenectomy. Two principal techniques are currently employed: the Kimura technique, which preserves the splenic artery and vein, and the Warshaw technique, which sacrifices these vessels and relies on short gastric vessels for splenic perfusion. With advances in minimally invasive surgery, reassessment of the optimal surgical strategy is warranted.
Methods
We reviewed recent evidence comparing the Kimura and Warshaw techniques in SPDP, focusing on perioperative outcomes, splenic perfusion–related complications, and long-term preservation of splenic function. Data from systematic reviews, meta-analyses, and international multicenter studies were evaluated.
Results
Major perioperative outcomes, including overall morbidity, severe complications (Clavien–Dindo grade ≥III), and mortality, were comparable between the two techniques. However, splenic perfusion–related complications—such as splenic infarction, development of gastric collateral circulation or gastric varices, and secondary splenectomy—were consistently less frequent in patients undergoing the Kimura technique. Long-term survival was similar, but splenic-related morbidity was higher after the Warshaw technique. Preservation of splenic blood flow was associated with better maintenance of splenic parenchyma and immunological function.
Conclusions
Although both techniques provide acceptable perioperative safety in SPDP, the Kimura technique demonstrates clear superiority in long-term qualitative outcomes related to splenic perfusion and function. For benign or low-grade malignant pancreatic lesions, splenic vessel preservation should be prioritized whenever technically feasible. A “Kimura-first” strategy, with conversion to the Warshaw technique only when necessary, represents a rational and evidence-based approach in contemporary minimally invasive pancreatic surgery.
Editorial
**A "Kimura-First" Strategy for Spleen-Preserving Distal Pancreatectomy:Reconsidering the Optimal Surgical Philosophy**
Tokyo Metropolitan Kasukabe Hospital
Hospital President
Wataru Kimura, MD, PHD
Spleen-preserving distal pancreatectomy (SPDP) has long been advocated for benign and low-grade malignant pancreatic tumors to avoid the well-recognized infectious and immunological consequences of splenectomy. Two distinct techniques-the Kimura technique with preservation of the splenic artery and vein, and the Warshaw technique relying on short gastric vessels after splenic vessel division-have been widely adopted. Although both techniques are considered technically acceptable, the fundamental question remains: which strategy should be prioritized in contemporary pancreatic surgery?
Accumulating evidence now supports a clear answer. While perioperative safety profiles of the Kimura and Warshaw techniques are largely equivalent, qualitative long-term outcomes related to splenic perfusion and function consistently favor the Kimura technique. Systematic reviews and meta-analyses have repeatedly demonstrated lower rates of splenic infarction, gastric collateral circulation, gastric varices, and secondary splenectomy when splenic vessels are preserved. These differences are not trivial complications but clinically meaningful events that may manifest years after surgery and necessitate prolonged surveillance or additional interventions.
The philosophical distinction between the two techniques is crucial. The Warshaw technique accepts altered splenic hemodynamics as an inherent trade-off to avoid splenectomy, whereas the Kimura technique seeks to preserve both anatomical integrity and physiological splenic function. In an era increasingly focused on quality of survivorship rather than short-term safety alone, preservation of normal splenic blood flow should be regarded as a fundamental surgical objective rather than an optional refinement.
Importantly, technical feasibility can no longer be cited as a major limitation. Advances in laparoscopic and robotic surgery have significantly expanded the ability to safely dissect and preserve the splenic vessels, even in challenging anatomical settings. Recent reports describing robotic SPDP emphasize a pragmatic and reproducible strategy: initially attempt the Kimura technique, convert to the Warshaw technique only if splenic vessel preservation proves unsafe or impossible, and reserve splenectomy strictly as a last resort. This stepwise approach reflects not only technical maturity but also a shift in surgical philosophy toward organ- and function-preserving surgery.
From an immunological standpoint, morphological preservation of the spleen alone may be insufficient. Maintenance of adequate splenic perfusion is likely essential for preserving immunological competence, particularly against encapsulated organisms. Thus, a "Kimura-first" strategy aligns with both anatomical logic and immunological principles.
In conclusion, current evidence supports redefining the standard approach to SPDP. The Kimura technique should no longer be viewed as merely one option among many, but rather as the default first-line strategy for benign and low-grade malignant pancreatic lesions. The Warshaw technique remains a valuable and appropriate fallback option when vessel preservation is not feasible, but it should not be the starting point. Adoption of a "Kimura-first" strategy represents a rational, evidence-based evolution in spleen-preserving pancreatic surgery, placing long-term organ function and patient-centered outcomes at the forefront of surgical decision-making.
Short Editorial
Why "Kimura-First" Should Be the Default Strategy in Spleen-Preserving Distal Pancreatectomy
Tokyo Metropolitan Kasukabe Hospital
Hospital President
Wataru Kimura, MD, PHD
Spleen-preserving distal pancreatectomy (SPDP) represents one of the clearest examples of how surgical philosophy has evolved beyond technical feasibility toward preservation of long-term organ function. Although both the Kimura and Warshaw techniques have been accepted as valid approaches, growing evidence suggests that they should not be regarded as equivalent choices. Instead, contemporary data support a clear hierarchy: the Kimura technique should be attempted first, with the Warshaw technique reserved as a secondary option.
Historically, the Warshaw technique gained popularity because it simplified the procedure by avoiding meticulous dissection of the splenic artery and vein. By relying on short gastric vessels for splenic perfusion, surgeons were able to preserve the spleen while reducing operative complexity. However, this approach inherently accepts altered splenic hemodynamics as an unavoidable compromise. In contrast, the Kimura technique is based on a fundamentally different concept: preservation of both splenic anatomy and physiology through maintenance of normal arterial inflow and venous drainage.
Recent systematic reviews and meta-analyses have clarified that this conceptual difference has tangible clinical consequences. Although major perioperative outcomes-such as overall morbidity, severe complications, and mortality-are comparable between the two techniques, splenic perfusion-related complications occur significantly more frequently after the Warshaw technique. These include splenic infarction, development of gastric collateral circulation and gastric varices, and the need for secondary splenectomy. Importantly, these complications are often delayed and may emerge long after the immediate postoperative period, undermining the apparent short-term equivalence of the two approaches.
The clinical relevance of these findings should not be underestimated. Splenic infarction can cause chronic pain, fever, or abscess formation, while gastric varices may necessitate lifelong surveillance and carry a risk of bleeding. Secondary splenectomy, although relatively uncommon, negates the original intent of spleen preservation and exposes patients to infectious risks that SPDP was designed to avoid. When viewed through the lens of long-term patient-centered outcomes, these events represent a meaningful disadvantage.
From an immunological perspective, preservation of splenic tissue alone may be insufficient. The spleen plays a critical role in immune defense against encapsulated organisms, and adequate perfusion is likely essential for maintaining this function. The Warshaw technique, by design, compromises venous outflow and alters microcirculation within the spleen. While many patients remain asymptomatic, the physiological cost of this compromise should not be dismissed as trivial. The Kimura technique, by preserving splenic vessels, aligns more closely with the principle of true functional organ preservation.
One might argue that the Kimura technique is technically demanding and not always feasible. This argument, however, is increasingly outdated. Advances in laparoscopic and robotic surgery have markedly improved visualization, dexterity, and precision in vascular dissection. Recent robotic series have demonstrated that splenic vessel preservation can be safely achieved in a majority of patients, even in complex anatomical settings. These studies consistently advocate a stepwise approach: attempt the Kimura technique first; if splenic vessel preservation is unsafe, convert to the Warshaw technique; and reserve splenectomy as a last resort.
This "Kimura-first" strategy reflects a mature surgical philosophy. It acknowledges technical reality without abandoning the goal of optimal long-term outcomes. Importantly, it does not reject the Warshaw technique; rather, it repositions it appropriately-as a valuable fallback option rather than a default choice. In an era where surgical success is increasingly measured by quality of survivorship, it is no longer sufficient to focus solely on perioperative safety. Surgeons must consider the lifelong implications of altered anatomy and physiology. SPDP offers a unique opportunity to preserve both the spleen and its function, but this opportunity is fully realized only when splenic vessels are preserved whenever possible.
In conclusion, the Kimura technique should be regarded as the standard first-line approach in SPDP for benign and low-grade malignant pancreatic lesions. A "Kimura-first" strategy is not merely a technical preference but an evidence-based commitment to preserving normal physiology, minimizing long-term complications, and prioritizing patient-centered outcomes. The Warshaw technique remains an important and appropriate alternative-but it should no longer define the starting point of spleen-preserving pancreatic surgery.
Reviewer Anticipated Q&A
Why not a Warshaw-first strategy?
Q1. The Warshaw technique is simpler and faster. Why not use it as the default approach?
A. Simplicity alone should not define the default strategy. Although perioperative outcomes are similar, multiple studies demonstrate higher rates of splenic perfusion-related complications after the Warshaw technique. These delayed complications directly affect long-term patient outcomes and justify prioritizing splenic vessel preservation whenever feasible.
Q2. Many patients undergoing the Warshaw technique remain asymptomatic. Are these complications clinically meaningful?
A. Yes. Splenic infarction, gastric varices, and secondary splenectomy are not trivial findings. They may require prolonged follow-up, additional interventions, or late reoperation. Their delayed nature does not diminish their clinical significance.
Q3. Is splenic function truly compromised after the Warshaw technique?
A. While definitive functional testing is limited, immunological principles strongly suggest that adequate splenic perfusion is necessary for optimal function. Preservation of splenic blood flow in the Kimura technique provides a physiological advantage consistent with the goals of organ-preserving surgery.
Q4. Isn't the Kimura technique technically demanding and potentially unsafe in difficult cases?
A. Technical difficulty alone does not justify abandoning an optimal strategy. With modern laparoscopic and robotic platforms, splenic vessel preservation is increasingly achievable. A Kimura-first strategy does not mandate vessel preservation at all costs; it allows conversion to the Warshaw technique when safety is compromised.
Q5. Should the Warshaw technique still be used?
A. Absolutely. The Warshaw technique remains a valuable alternative when splenic vessel preservation is not feasible. However, it should be considered a secondary option rather than the initial strategy.